After a series of spine surgeries left a 69-year-old man reliant on a wheelchair or cane, multiple centers were unable to help his complex case: a partially fused spine with a forward/side-leaning stoop which also compressed nerves, causing sciatic leg pain. Additionally, a previous weight-loss surgery complicated his presentation. The patient was no longer able to enjoy time with his grandchildren, fish on his boat, or take a walk on the beach with his wife.
After consulting several other surgeons who could not help him, the patient came to Brett Rocos, MD, for revision spine surgery. “No amount of physical therapy or increasing muscle strength would have been enough to correct this patient’s spine,” Rocos says. “We’re the last line for patients like this. Either we do it or no one does.”
How did Rocos correct the patient’s previous surgeries?
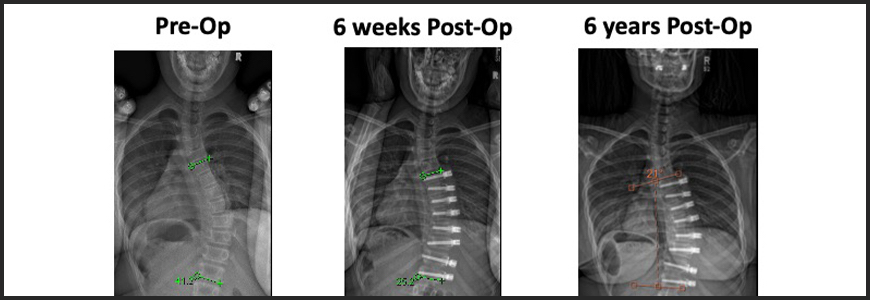
In a nine-hour surgery, Rocos and the team began by removing previous devices from a lumbar fusion and a spinal cord stimulator. They then decompressed the spine and placed artificial bone grafts between the vertebrae. Using four cobalt rods and approximately 40 screws from T2 to the pelvis, the team pulled the patient’s spine straight. “We recreated normal spine anatomy as best we could,” says Rocos.
Rocos reports that the patient was able to stand the day after surgery. His healing was complicated by a serious infection, but Duke critical care and infectious disease teams coordinated with his previous weight-loss surgeon to provide high-quality care for a full recovery.
Rocos cites the coordinated care teams as critical to this patient’s success. “I’ve never been anywhere where we work so closely with our critical care teams,” Rocos says. “The attending relationships are superb.”
With hundreds of years of combined experience and internationally recognized experts within the faculty, Duke physicians have seen every shape and severity of spine deformity. Within the spine division and across the three hospital campuses of the Duke system, Rocos says the faculty has access to every technology in spine surgery: “Not just surgical and imaging technology but also perioperative tech, all backed by a huge support team behind the acute clinical care.”
With the help of these coordinated teams, the patient is now able to walk and move independently again. A year after his surgery, the patient has returned to the outdoor activities he previously enjoyed. His fishing catches have gone viral on social media.
“My work is very much this type of last resort,” says Rocos. “This patient’s journey reflects the path for these complicated cases. He epitomizes what I’m here to do.” Rocos will expand his work to include pediatric spine cases.
For Orthopaedic Spine referrals, call 919-613-7797.
For Neurosurgery Spine referrals, call 919-684-7777.