The increasing use of automated measuring devices, ambulatory monitoring, and a trend toward more at-home measurements may help reduce inconsistent blood pressure (BP) readings that can create confusion among patients and potentially affect long-term health outcomes.
Consistent, accurate data is particularly important to create treatments plans for high-risk patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD).
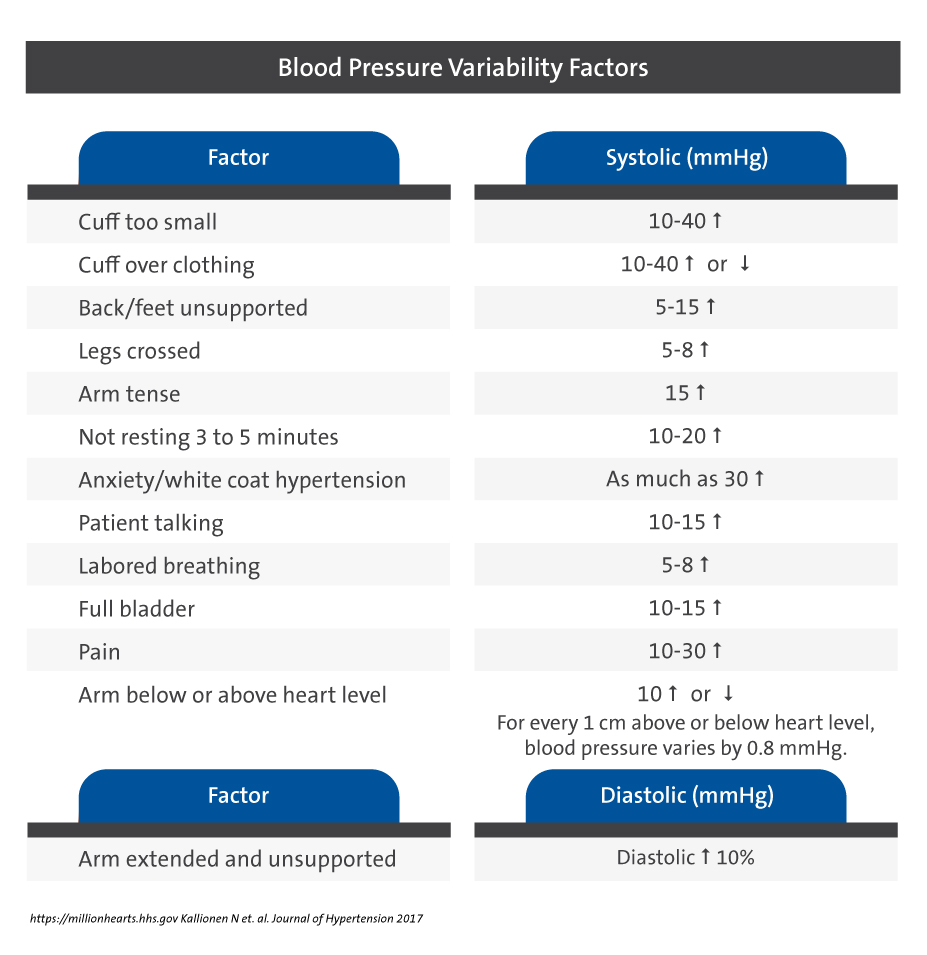
Inaccurate measures are common in busy clinics where BP readings can be influenced by tactics, equipment, or temporary patient circumstances, says Crystal Tyson, MD, a Duke nephrologist who specializes in treating hypertension. Inaccurate readings have two significant consequences: misdiagnosis and inadequate or inappropriate prescribing.
Emerging research into the consequences of inaccurate BP measurement as well as the effectiveness of new devices will help clinicians, Tyson says. A University of Pennsylvania Hospital nephrologist and researcher, Jordana B. Cohen, MD, MSCE, urges clinicians to use the latest measuring devices to ensure more precise BP measures. Cohen’s research is performed in conjunction with the Renal, Electrolyte and Hypertension Division at the University of Pennsylvania and the University of Pennsylvania’s Center for Clinical Epidemiology and Biostatistics.
“Physicians do not always have the time or support to perform the highest quality readings,” says Cohen, who recently presented her laboratory’s research with Duke Nephrology Division faculty. “But we need to do a lot better and we can do a lot better.”
Sophisticated analyses of longitudinal patient data indicate a need for better control of hypertension, which requires more precise BP measurement, Cohen says. Cohen also urges clinicians to consider the possibility and consequences of masked, uncontrolled, or white coat hypertension.
To achieve greater accuracy in BP measures, Cohen recommends several new approaches:
Automated Office BP Measurement (AOBP): With a single activation, an oscillometric device records multiple BP readings after a rest period for the patient. The devices are pre-programmed for a five-minute rest, then three readings at one-minute intervals.
24-hour Ambulatory Blood Pressure Monitoring (ABPM): Records BP during a full day of routine patient activity. Research shows that APBM is a greater prognostic indicator of longitudinal cardiovascular outcomes.
Home (self-measured) BP Monitoring (HBPM): Improves upon in-office BP measurement by eliminating the white coat effect. This option is ideal for longitudinal out-of-office BP monitoring due to easy access to monitors and simplicity of interpretation.
However, Cohen notes that there is inadequate evidence to support using HBPM as opposed to ABPM for predicting cardiovascular disease and mortality.