When it comes to managing the debilitating symptoms of osteoarthritis (OA), the Duke Joint Health Program (JHP) has taken traditional efforts to the next level—designing, implementing, and tracking a longitudinal lifestyle and behavioral health modification program for patients with hip and knee OA.
This personalized program brings together a team of orthopaedic surgeons, physical therapists, dietitians, bariatricians, endocrinologists, psychologists, and pain management specialists to develop comprehensive care plans that create long-term improvements in their joint health and prepare patients psychologically and physically for possible surgery, if needed. While the length of active participation is personalized to a patient’s goals and underlying condition and can last anywhere from a few months up to one year, the JHP remains a resource that the patient can return to should they need it throughout their life.
“As a joint surgeon, I know that many arthritis patients do not need surgery initially, and I was frustrated by our lack of a more comprehensive OA program,” says William A. Jiranek, MD, JHP co-founder.
Research by JHP co-founder and orthopaedic surgeon Richard C. Mather, MD, MBA, and others has shown that people with significant psychosocial problems have difficulty managing the symptoms of arthritis in addition to having a much harder time recovering from surgery, often with poorer results. The JHP marries the physical therapy and musculoskeletal conditioning part of arthritis care with identifying and helping patients with associated psychosocial comorbidities affecting their treatment through cognitive behavioral theory-based strategies.
Since its inception in October 2017, more than 1,300 patients have enrolled in this collaborative program led by Duke’s Department of Orthopaedics and the Department of Physical Therapy and Occupational Therapy. The JHP’s offerings have also grown exponentially—from one provider at one location to 14 providers at 12 locations in North Carolina.
The secret ingredient: POPs
Primary osteoarthritis providers (POPs) are Duke orthopaedic physical therapists with extensive musculoskeletal training in hip and knee OA who are further trained in holistic approaches to nutrition and weight management, sleep quality, psychological distress, and cognitive behavioral theory-based strategies as they relate to OA and pain. Because of the POPs’ specialized training in these areas, patients can be referred to one person who then provides treatment or coordinates appropriate referrals.
POPs frequently follow up with patients using MyChart, phone calls and/or e-mail to assess their functionality, pain levels, and psychological distress, helping to drive personalized changes and improvements to their care plan.
“The Joint Health Program really allows for every relevant provider to be operating at the top of their license,” says Jonathan O’Donnell, MD, business manager for the Duke JHP. “These follow-up touchpoints help us to effectively engage patients outside of the four walls of the healthcare space and into their own lives, communities, and homes.”
Tracking preoperative progress
POPs use a “yellow-flag” tool developed in a study by Duke physical therapists to assess 11 psychological constructs measuring pain-associated psychological distress. O’Donnell says this measure estimates in 10 questions what would take more than 136 questions in other surveys, and covers negative mood, fear avoidance behavior, and pain coping skills—“three important domains that are fundamental to the work we’re trying to do,” he says. Compared with common tools such as the Patient Health Questionnaire-9 or the Pain Catastrophizing Scale, “we feel this tool is a useful way to clinically apply research knowledge and actually use it to guide clinical decision-making,” O’Donnell adds.
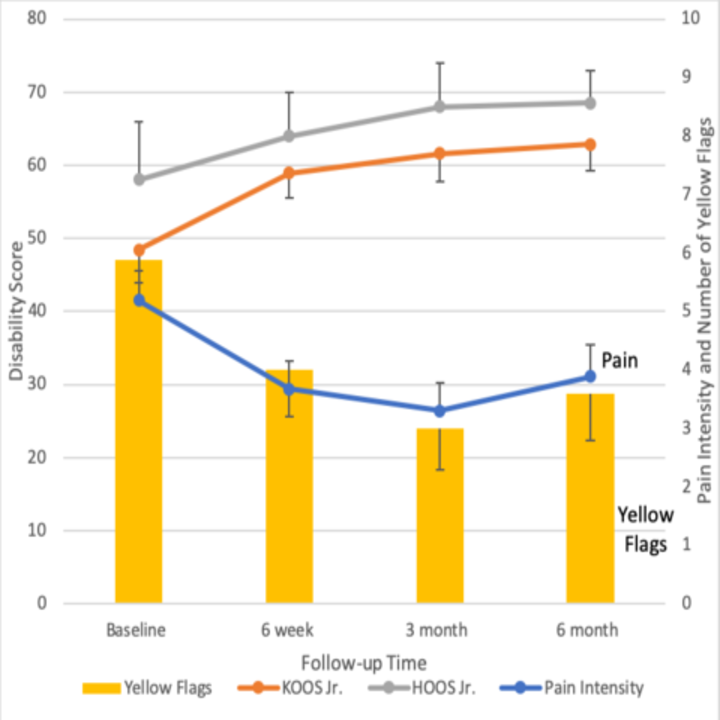
The JHP also tracks KOOS Jr., HOOS Jr., and pain intensity levels. “Our data indicate that we are improving some of the pain-associated psychological distress patients have and that their patient-reported functional outcome scores have improved substantially,” Jiranek says. In addition, the data show that many patients have delayed surgery or feel they no longer need it by supplementing their arthritis treatment with this comprehensive care approach.
The chart below shows disability, pain intensity, and yellow-flag values over time for patients completing all follow-up in the Duke JHP (n=86).