Finding the Right Treatment for Spinal Stenosis

FIGURE 1. Radiography shows mild compression fracture and spondylolisthesis
A 73-year-old man with a history of chronic axial back pain presented to his primary care physician after his pain worsened and he began experiencing weakness and paresthesia in his lower extremities that made it difficult to walk.
During his many years with back pain, he had tried home-exercise programs, physical therapy, and medical management, but the condition persisted. When he lost his ability to effectively ambulate and carry out his daily activities, he knew he had to find a new solution. His physician referred him to Duke spine surgeon Seth Hayes, MD, who focuses on using minimally invasive approaches and innovative technology to decrease complications and optimize outcomes.
Radiography of the spine performed at Duke revealed a mild compression fracture at the L5 vertebra and slight spondylolisthesis at L4 and L5 (Figure 1), in addition to severe spinal stenosis.
Question: What new option did Hayes offer the patient to ameliorate his pain and help him maintain mobility?
Answer: Hayes performed a procedure using a coflex Interlaminar Stabilization device (Paradigm Spine, New York, NY), a titanium metal implant placed between the laminar bones to keep the spine stable after surgical decompression (Figure 2).
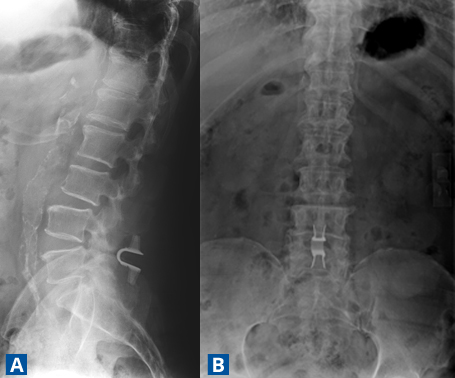
FIGURE 2A–B. (A) Lateral and (B) anteroposterior x-rays of the stabilization device
Historically, the patient’s only options would have been lumbar decompression back surgery, at the one extreme, or lumbar spinal fusion, on the other. However, the coflex Interlaminar Stabilization device, approved by the US Food and Drug Administration in 2012, offers a new option for treating back pain and nerve compression that minimizes the risk of recurrence in appropriately selected patients while allowing those patients to function without the loss of mobility that accompanies fusion surgery.
The procedure itself involves less blood loss and shorter operative times and hospital stays than spinal fusion, Hayes says.
“With fusion surgery, the recovery is generally several months,” he explains. “The recovery for this procedure is much quicker. Whereas before, this patient was having trouble standing for reasonable periods of time, walking, going to the grocery store, et cetera, within a few weeks of the procedure, he had significant improvement in his lower back pain, and his lower-extremity and walking issues had been resolved.”
As part of Hayes’ approach to help patients avoid back pain in the future, the patient is participating in postoperative physical therapy. He has also minimized his need for medical management for his pain.
“This approach is not for everyone,” Hayes cautions. “But, for the right patient, especially someone who is older and has severe stenosis with significant neurogenic claudication/mechanical back pain but only minimal, low-grade spondylolisthesis, this can be a great way to provide stability and maintain range of motion, while avoiding fusion.”
Furthermore, if this approach fails to relieve the patient’s pain or problems with ambulation, Hayes notes, then the patient is still a candidate for fusion.